Deep Work for Physicians: Protecting the Cognitive Core of Medicine
Deep work is not a productivity hack for doctors. It is a clinical safety issue, a training issue, and a systems design issue. Physicians need to protect deep thinking and automate the shallows.
Listen to this post
Deep Work for Physicians: Protecting the Cognitive Core of Medicine
Last week I was working through a complex maternal-fetal medicine consultation when the usual parade began. A refill request. A portal message. A secure chat ping. A chart alert that was technically relevant and cognitively useless.
None of those interruptions were catastrophic on their own. Together, they broke the part of the work that actually mattered.
That is the piece of medicine we keep failing to protect.
The Framing Is Wrong
When physicians talk about focus, we often talk about it as if it were a personal discipline problem. We tell ourselves to be more efficient, triage faster, clear the inbox sooner, and somehow think more deeply in the margins.
The framing is wrong.
Deep work for physicians is not a lifestyle upgrade. It is not aesthetic productivity. It is the set of conditions required for serious clinical judgment.
Medicine is knowledge work with a human cost for distraction. Differential diagnosis is deep work. Ultrasound interpretation is deep work. Synthesizing a consult note that reflects what you actually think is deep work. Counseling a family through uncertainty without collapsing into canned language is deep work.
If the system keeps physicians in a state of forced shallowness, the system is not merely inefficient. It is hostile to good medicine.
Physicians Were Reclassified Into Shallow Workers
Cal Newport’s original argument still holds in 2026: the ability to focus without distraction is becoming more rare and more valuable. His update is even sharper. Focus is a form of cognitive fitness. If you stop training it, it weakens.
Physicians should hear that as a warning.
The modern EHR environment has quietly reclassified doctors. We were trained as diagnosticians, synthesizers, and knowledge workers. In practice, many of us now function as high-cost interruption processors moving between inboxes, refill queues, prior authorizations, secure messages, attestation clicks, and fragmented documentation tasks.
That is not just annoying. It changes what sort of mind the job is training.
Every time the day is organized around micro-responses instead of sustained thought, the profession gets better at shallow throughput and worse at deep judgment.
Shallow Medicine Has an Architecture
This problem persists because the architecture rewards interruption.
Patient portals reward immediate responsiveness. Secure chat rewards the sender, not the interrupted clinician. EHR alerts are tuned to legal and operational anxiety, not cognitive load. Administrative workflows keep routing clerical drag toward the physician because the physician is the most reliable human exception handler in the building.
No single feature has to be malicious for the aggregate effect to be destructive.
That is how shallow medicine works. It does not announce itself as an attack on physician attention. It arrives disguised as convenience, safety, compliance, throughput, patient engagement, and “just one quick message.”
Then it consumes the day.
What Deep Work Looks Like in Clinical Practice
Physicians do not need a vague defense of focus. We need a precise definition of what is being protected.
Deep clinical work includes:
- building a differential before the machine stages one for you
- reviewing imaging without a running commentary from the inbox
- writing the assessment and plan from actual synthesis instead of template inertia
- reading the literature closely enough to change how you practice
- thinking through edge cases, exceptions, and atypical presentations
- counseling patients when uncertainty is real and the answer is not in a dropdown
Shallow clinical work includes:
- inbox triage
- routine refill processing
- prior authorization logistics
- compliance attestations
- duplicated documentation steps
- message routing that should have been solved upstream in workflow design
Shallow work is not evil. Some of it is necessary. The problem is allocation. We keep spending prime cognitive hours on work that barely requires physician judgment, then acting surprised when the deep work gets pushed into evenings, weekends, and emotional exhaustion.
Cognitive Fitness Matters for Doctors More Than Most People
Newport’s 2026 update on cognitive fitness matters in medicine because our errors are not abstract.
If you spend your day training rapid context switching, fragmented reading, and reflexive response behavior, you are practicing a cognitive style. That style becomes normal. It becomes easier to scan than to think, easier to verify than to generate, easier to react than to reason.
That is dangerous for experienced physicians. It is even more dangerous for trainees.
Residents and fellows develop judgment by struggling through ambiguity before certainty arrives. If every difficult task begins with an AI summary, a protocol recommendation, or a machine-generated first pass, the immediate output may improve while the deeper professional capability erodes.
That is the real risk. Not that machines can help. That physicians will stop exercising the reasoning muscles the profession depends on.
The Anti-AI Rule Physicians Need
This is where the conversation has to become more disciplined.
AI should aggressively remove shallow administrative work. It should summarize records, compress inbox noise, draft low-stakes operational language, and pull forward structured context that saves physicians time.
But physicians should be extremely careful about outsourcing original clinical thought.
The struggle to write the assessment is often the act of clarifying the assessment. The effort of explaining a plan in your own words is often the act of discovering whether the plan is coherent. If you skip straight to generated reasoning, you may save minutes while losing formation.
I use AI. I build with AI. I am not interested in purity rituals.
I am interested in preserving the physician mind.
That means using machines hardest on the shallows and keeping humans firmly responsible for the work that creates judgment: first-pass reasoning, synthesis, interpretation, prioritization, and moral accountability.
Why This Is a Builder Problem
This is where Doctors Who Code becomes relevant.
Deep work for physicians cannot depend only on personal willpower. No amount of discipline fixes a workflow designed to fracture attention. This is a systems problem, which means it is also a design problem.
We need better architectures:
- inboxes processed in batches instead of ambiently
- pre-visit summaries that reduce chart reconstruction time
- note pipelines that remove clerical friction without replacing physician interpretation
- escalation pathways that stop routing every edge case to the doctor by default
- local or supervised AI systems that automate drudgery without quietly owning the reasoning loop
That is what physician-builders should be doing.
The goal is not to make doctors faster at clicking through broken systems. The goal is to build systems that stop wasting physician cognition in the first place.
That is why I keep coming back to workflow tools, documentation pipelines, and narrow automation. They are not side projects. They are cognitive defense infrastructure.
A Practical Deep Work Protocol for Physicians
If you want a starting point, make it operational.
- Protect one or two daily blocks for actual thinking. Chart review, consult synthesis, imaging review, literature reading, or technical building work. Close the inbox during those blocks.
- Batch portal and inbasket work into defined windows. Do not let message triage become the ambient soundtrack of clinical reasoning.
- Turn off every alert that is not truly urgent. If the system screams constantly, it is training you to ignore signal.
- Keep the phone off the desk during patient encounters and focus blocks. Presence matters. So does friction against compulsive checking.
- Use AI for summarization, retrieval, formatting, and first-pass administrative compression. Do not let it become your replacement for first-pass thought.
- Preserve one recurring block each week for learning or building. Read deeply. Write. Prototype. Think. Physicians who never protect cognitive depth eventually forget what it feels like.
None of this is magical. It is simply a refusal to surrender the best hours of the physician mind to low-yield interruption.
What Is Actually at Stake
Burnout is part of this story, but it is not the whole story.
What is at stake is the intellectual identity of the physician.
If medicine becomes a profession that mainly reviews generated summaries, validates machine suggestions, responds to asynchronous noise, and manages software designed by people who do not understand clinical reasoning, then we will still look busy. We will still look modern. We will also be less capable.
I do not think physicians need nostalgia. I think we need standards.
We should demand systems that protect deep thought. We should train doctors to think before the model speaks. We should automate the clerical burden hard and without apology. We should treat sustained clinical reasoning as a resource worth defending at the architectural level.
Deep work for physicians is not optional.
It is part of how good medicine still happens.
If we do not protect it, the inbox will happily take its place.
Related Posts
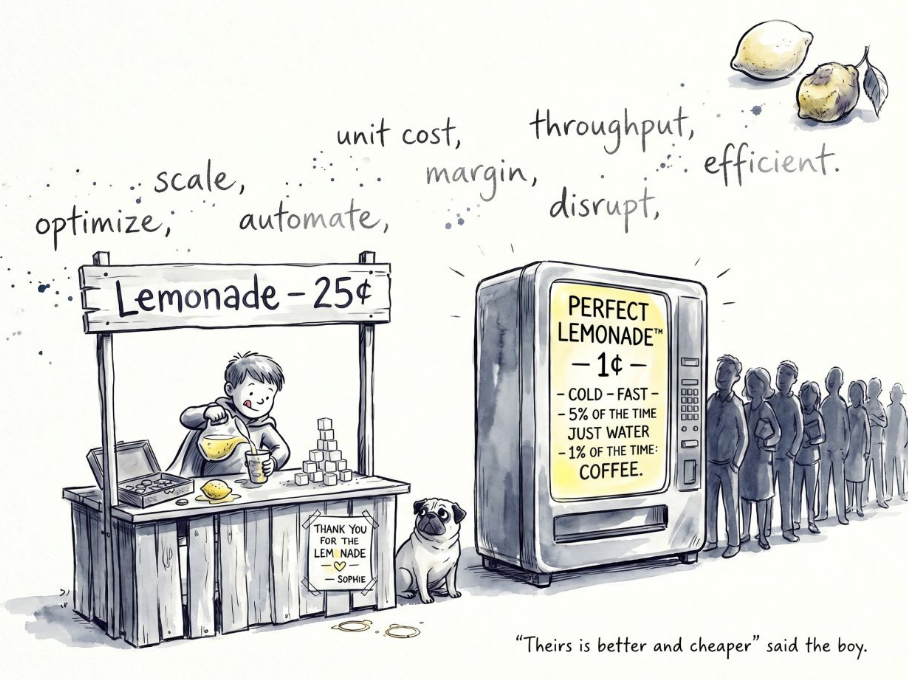
The Lemonade Machine Problem
Automation in medicine should not be judged against an ideal clinician. It should be judged against real human variance, machine variance, supervision, and the cost of failure.
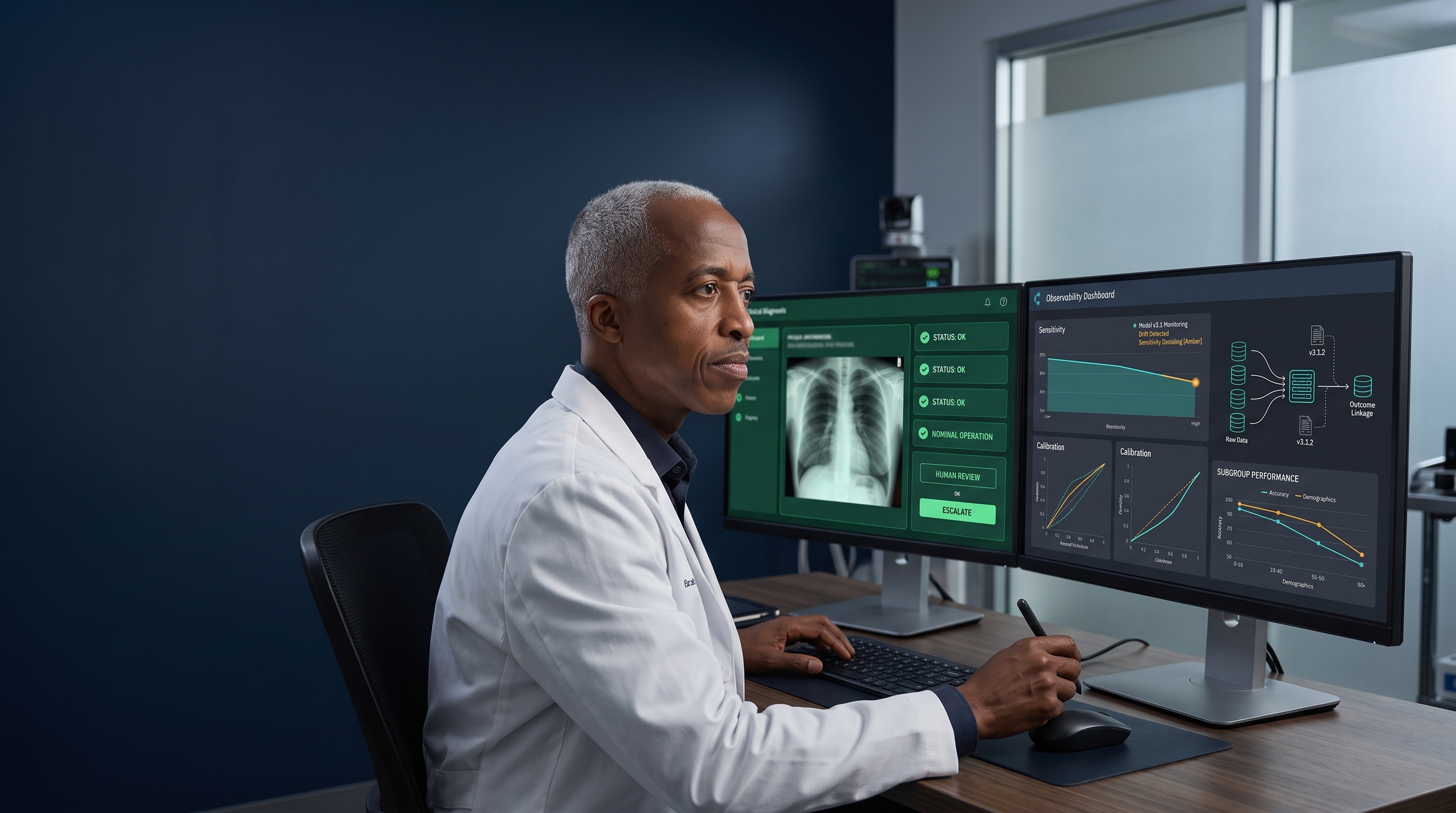
FDA Clearance Is Not a Monitoring Plan
Clinical AI can fail without crashing. Physician-developers must build the monitoring, outcome linkage, and human checkpoints that keep cleared software safe after deployment.
From Meetings to Modules: Redefining Clinical Coordination
Clinical teams do not move slowly because clinicians are slow. They move slowly because pages, meetings, and verbal handoffs force physicians to keep re-explaining decisions that software should carry forward.

Maternal-Fetal Medicine Specialist