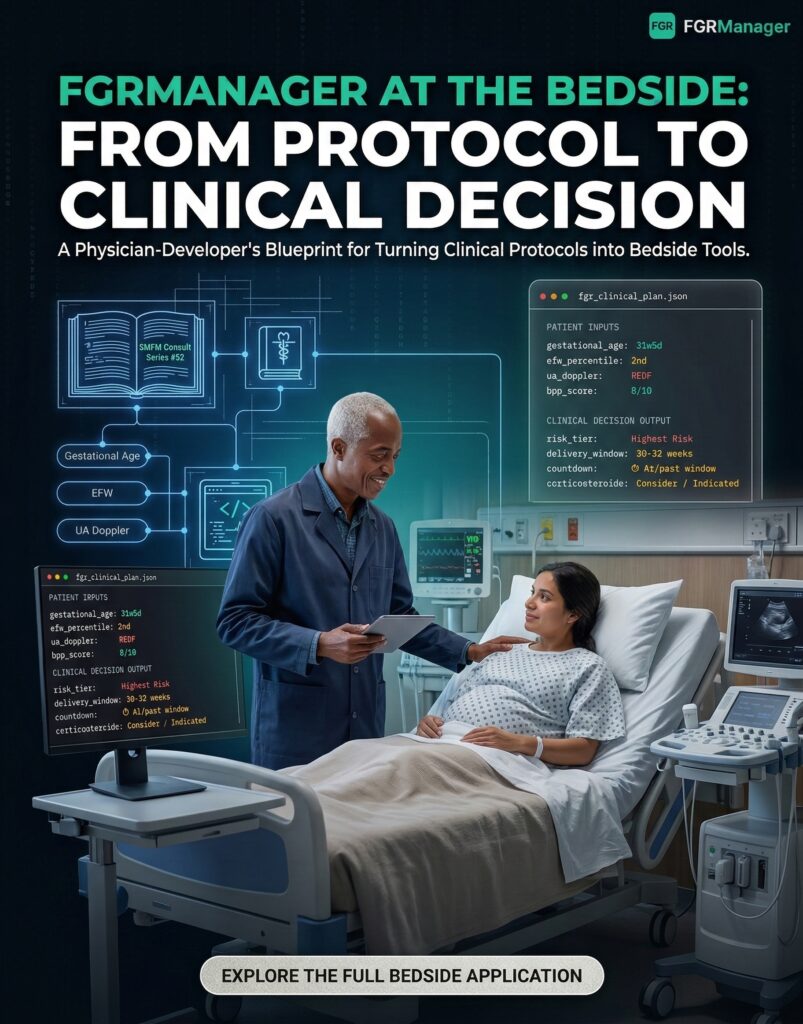
GitHub Gists: The Most Underrated Tool Every Physician-Developer Should Be Using
GitHub Gists look like scratch space for code snippets. Used correctly, they become a version-controlled clinical reference library that decks, apps, and blog posts can all cite from a single source.
· 9 min read