RAG Is the Bridge Between Medical Knowledge and Medical Practice
Clinical AI earns workflow trust only when its answers are grounded in current, local, auditable knowledge. Retrieval is not a feature. It is infrastructure.
Listen to this post
RAG Is the Bridge Between Medical Knowledge and Medical Practice

The answer sounded right.
That was the problem.
It had the cadence of medical confidence without the burden of local knowledge.
A clinician asked an AI system a practical question about a departmental protocol. The answer was fluent. It named the condition, summarized the management, and presented the steps in a sequence that looked usable.
Then someone checked the actual protocol.
The local pathway had changed.
The model knew the medical language. It did not know the hospital.
That distinction is where clinical AI becomes dangerous.
The Model Does Not Know Your Hospital
A general-purpose model can know a great deal about medicine.
It can explain preeclampsia. It can summarize fetal growth restriction. It can describe diabetes in pregnancy. It can compare screening strategies, outline counseling points, and produce language that sounds clinically mature.
That is useful.
It is also incomplete.
Clinical practice depends on the last mile.
Which protocol does this department use?
Which formulary restriction applies?
Which ultrasound workflow changed last quarter?
Which referral pathway is currently active?
Which template is required for documentation?
Which attending preference is actually a departmental standard and which one is just habit?
The model does not know these things by default.
It may know the broad medical concept and still fail the workflow.
That is not a small failure. A locally wrong answer can be more dangerous than an obviously absurd one because it is easier to trust.
Clinical AI cannot be judged only by whether the answer sounds medical.
It must be judged by whether the answer is grounded.
Static Knowledge Is the Wrong Container
Static knowledge fails quietly in clinical environments.
A PDF gets updated. The old version remains on a shared drive. A protocol gets revised after a quality review. The screenshot in someone’s teaching folder remains unchanged. A formulary restriction changes, but the handout still reflects last year’s practice.
This is not unusual.
This is normal clinical knowledge behavior.
The problem is that many AI tools treat knowledge as if it were stable. They answer from training data, pasted context, or a one-time document upload. That can work for generic explanation. It fails for operational medicine.
Guidelines change.
Local implementation changes faster.
The messy last mile is where clinical practice actually happens.
Formularies. Templates. Staffing patterns. Ultrasound slots. Preference cards. Referral pathways. Prior authorization requirements. Departmental consensus. EHR limitations.
These are not footnotes.
They are the operating system of care.
If the AI system cannot reach that layer, it is not ready for workflow trust.
The Knowledge Grounding Test
The Knowledge Grounding Test is simple.
A clinical AI answer is not ready for workflow use unless it can show what source it used.
It must show when that source was last updated.
It must show which local protocol or institutional rule applies.
It must show where the clinician should verify the claim.
It must show what it does not know.
This is not a demand for perfect AI.
It is a demand for traceable AI.
A physician does not need a model to sound confident. Medicine already has enough confident voices. A physician needs the system to expose the basis of its answer so the human checkpoint can do its work.
That means retrieval is not decoration.
Retrieval is architecture.
What RAG Actually Does
Retrieval-augmented generation sounds more complicated than it is.
RAG gives the model a way to consult a curated knowledge base at the moment of the question.
The system ingests source documents.
It breaks them into retrievable units.
It converts those units into embeddings.
It stores them in a searchable index.
When the clinician asks a question, the system retrieves the most relevant material and gives it to the model as context.
The model then generates an answer grounded in those sources.
The important word is not “generates.”
The important word is “grounded.”
Without retrieval, the model is answering from general memory. With retrieval, it can answer from the department’s actual protocol, the current formulary document, the updated referral pathway, or the Markdown note that a physician-builder curated after the last committee meeting.
That changes the clinical meaning of the tool.
The AI surface may look like a chatbot.
The product is the knowledge infrastructure underneath it.
Curation Is the Product
Most people evaluating clinical AI stare at the interface.
The interface is the least interesting part.
The real product is the maintained knowledge base.
Which documents are included?
Who owns them?
How are they updated?
How are stale sources retired?
How are contradictions handled?
How does the answer show provenance?
How does the clinician verify the claim in under thirty seconds?
Those questions determine whether the system deserves trust.
For physician-developers, this is where tools like Obsidian, Markdown, and file-based knowledge systems matter. A department can maintain protocol notes in plain text. It can process PDFs into structured Markdown. It can keep source files under version control. It can build a retrieval layer over documents that physicians actually understand.
This is why I have written about the PDF wall in clinical RAG and why Docling matters. Bad document processing poisons everything downstream. A scrambled PDF becomes a scrambled chunk. A scrambled chunk becomes a plausible but wrong answer.
Retrieval quality begins before retrieval.
It begins with source discipline.
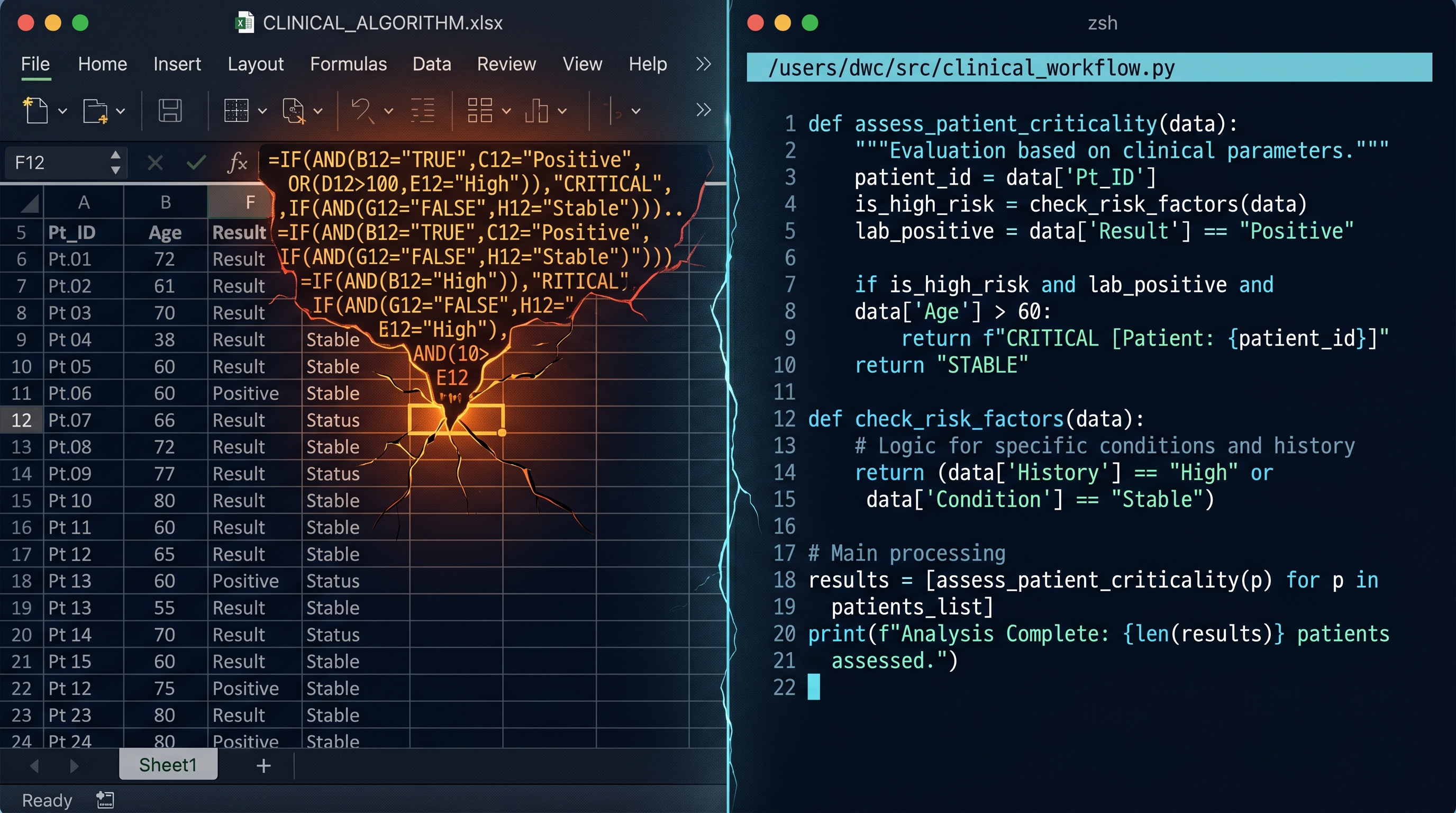
The Protocol Assistant Example
Imagine a department protocol assistant for obstetrics.
It contains local hypertension pathways, diabetes in pregnancy workflows, fetal growth restriction surveillance protocols, referral instructions, formulary guidance, patient handouts, and ultrasound scheduling rules.
A clinician asks:
For a patient at 32 weeks with fetal growth restriction and elevated umbilical artery Dopplers, what surveillance pathway should I follow here?A weak system answers from general obstetric knowledge.
A stronger system retrieves the local FGR protocol, the Doppler surveillance table, the date of the most recent departmental revision, and the page or section where the pathway lives.
Then it answers with citations.
It also says what it does not know.
It does not know the attending’s real-time clinical assessment. It does not know whether the patient has additional comorbidities unless those were provided. It does not know whether the ultrasound schedule has capacity today. It does not replace the clinician.
That is the correct shape.
The assistant should narrow the search space and expose the source. It should not pretend to be the final decision-maker.
The human checkpoint remains.
RAG Needs Tests Too
This series began with spreadsheets and moved through tests because clinical software discipline is cumulative.
RAG does not escape that discipline.
Retrieval should be tested.
If a clinician asks about the current magnesium sulfate protocol, the system should retrieve the current protocol, not an old lecture handout. If a query mentions fetal growth restriction with absent end-diastolic flow, the Doppler surveillance section should appear in the retrieved context. If a source is expired, the interface should show that clearly or remove it from the index.
Source freshness should be visible.
Hallucination checks should be built into the workflow.
The answer should cite the document. The citation should lead somewhere real. The system should make it easy for the clinician to verify the claim and hard for the model to hide uncertainty behind fluent language.
This is testing applied to knowledge.
The same logic that protects a calculator boundary protects a retrieval system. The tool must remember what good behavior looks like. It must fail visibly when the answer is not grounded.
The Bridge Is the Discipline
Clinical AI has a distribution problem.
The knowledge often exists.
It is just not available at the moment, in the right form, with the right provenance, under the right clinical pressure.
RAG is one bridge across that gap.
Not the only bridge.
Not a magic bridge.
A maintained, tested, source-aware bridge.
That is why physician-developers matter here. We know which details are clinically load-bearing. We know which protocol sections are dangerous when stale. We know which answers need a source and which answers need refusal. We know where the human checkpoint belongs.
The model is not the clinical memory.
The retrieval layer is.
Related Posts
The Moment a Clinical Tool Becomes Infrastructure
A short introduction to a DoctorsWhoCode series on spreadsheets, tests, and retrieval as the basic discipline of physician-built clinical software.
Why Your Clinical Calculator Needs Tests
A clinical calculator is not safer because it is written in code. It becomes safer when its expected behavior is explicit, checked, and protected from silent drift.
From Excel to Python: When Your Spreadsheet Becomes a Liability
Excel is often the right first move for a physician-builder. The problem begins when clinical logic stays trapped in a container that can no longer safely hold it.

Maternal-Fetal Medicine Specialist